Forming Labor-Management Partnerships for Systemic Change in Healthcare

Much has been written about the need for healthcare reforms in America.
Governmental attention is usually directed to increasing citizens’ access to insurance, to rewarding institutions for positive outcomes, or to penalizing institutions for practices that fall short—for example, for frequent and early hospital re-admissions. This top-down approach has been valuable in focusing hospital and systems administrators on essential bottom-line markers of effective treatments. Such approaches, however, need supplementation by finer-gauged methods for identifying and addressing the service gaps particular to each institution.
Governmental attention is usually directed to increasing citizens’ access to insurance, to rewarding institutions for positive outcomes, or to penalizing institutions for practices that fall short—for example, for frequent and early hospital re-admissions. This top-down approach has been valuable in focusing hospital and systems administrators on essential bottom-line markers of effective treatments. Such approaches, however, need supplementation by finer-gauged methods for identifying and addressing the service gaps particular to each institution.[1]
North American hospital administrators are rarely taught in business, medical, nursing, or public health schools how to meaningfully engage with clinicians or caregiving staff or with the unions that represent healthcare workers.[2] To the detriment of all, clinicians and other frontline staff are essentially told, “Keep your thoughts about patient care and the work environment to yourself. We know what’s best to keep this institution afloat.” This situation is particularly unfortunate in healthcare organizations, in which nurses, aides, pharmacists, dietary and cleaning personnel, physician assistants, and physicians can all observe problems in care delivery, in cost excesses, and in the uses of technology, and can contribute to solving them. When implemented effectively, frontline staff participation creates a co-generated process, weaving together the knowledge and skills of frontline staff and management to result in a stronger organization.[3]
This is true in every industry, but focusing on healthcare organizations is particularly important, as this is a growing sector of our national economy, and one that elicits significant concern due to skyrocketing costs and limited access to high-quality services. Healthcare costs now consume over 18 percent of our current gross domestic product (GDP),[4] and the healthcare sector is expected to generate more new jobs than most segments of the economy, at least through 2026.[5] The need for more coordinated, cost-effective services is also growing due to an aging population with patients who may have complex, intersecting illnesses such as diabetes, hypertension, autoimmune disorders, pulmonary diseases, and cardiac diseases.
Since healthcare services are mostly provided directly to patients on-site, aside from radiology and pathology, they cannot be outsourced,[6] which is a cost-cutting strategy used in other sectors of the U.S. economy. Thus, healthcare organizations must find different ways to cut costs while also providing high-quality-of-care outcomes.
It makes intrinsic sense for frontline providers and staff, who daily witness the aspects of their system that may not be cost-effective, to be enlisted in a joint effort toward cost containment.
THE IMPORTANCE OF LABOR-MANAGEMENT PARTNERSHIPS
In the United States, unions represent 20.7 percent of the healthcare sector’s workforce, a statistic that is increasing when union membership is shrinking in most other segments of our economy.[7] Any focus on employee participation within healthcare needs to take this fact into account. Happily, many unions representing healthcare workers[8] have themselves become increasingly sophisticated in working with healthcare administrators to create joint labor-management participation processes.
Modern healthcare organizations—outpatient clinics, inpatient settings, nursing homes—interface constantly with an array of insurance companies, each with its own set of costmonitoring practices, as well as with state and federal regulatory agencies. The need for these organizations to stay on top of the ever-changing regulatory and reimbursement processes has led to an increasing stratification within them, with CEOs, CFOs, and whole administrative branches devoted to budgeting and regulatory issues rather than to what happens within the hospital: patient care.[9] In fact, from 1975 to 2010, “[t]he number of healthcare administrators increased 3,200 percent. There are now roughly 10 administrators for every doctor within United States healthcare systems.”[10] In such topheavy organizations, administrators have become too far removed from the daily process of patient care to effectively manage all the issues that arise within their complex medical settings.[11]
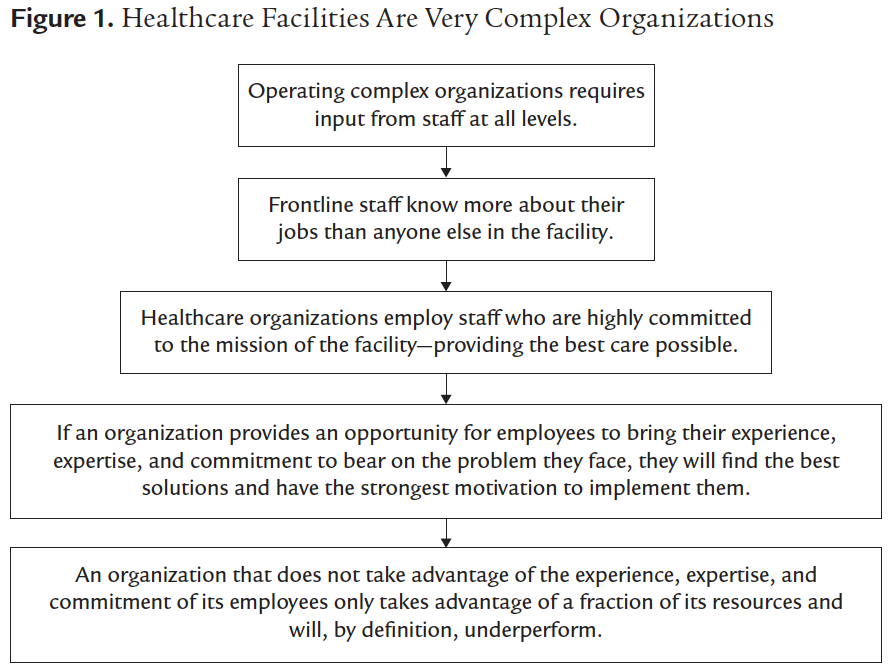
Complex organizations, as a rule, face real difficulty in making changes effectively and efficiently due to their having to face multiple variables, often occurring within siloed departments. It has become a common understanding in in the organizational studies literature that in complex institutions, the flexible but structured involvement of all key stakeholders is required to achieve an optimal result.[12] For healthcare organizations, this means that the staff who interact with and directly care for patients must be involved in decision-making processes—in analyzing both care-delivery shortcomings and opportunities for improvement. Working together, administrators and frontline staff can claim responsibility for envisioning, researching, and implementing the changes necessary to create a high-functioning complex organization devoted to caring for sick patients (see figure 1). At the unit and departmental levels especially, this involves consultation and knowledge sharing with all contributors to their particular mission.
The Labor-Management Partnership approach has emerged as especially useful in formalizing processes through which front-line staff can contribute to improving their workplaces while also making their own working lives more meaningful. The approach creates a clear process for frontline staff and administrators to jointly identify and solve patient care problems, make work decisions, and implement their solutions.
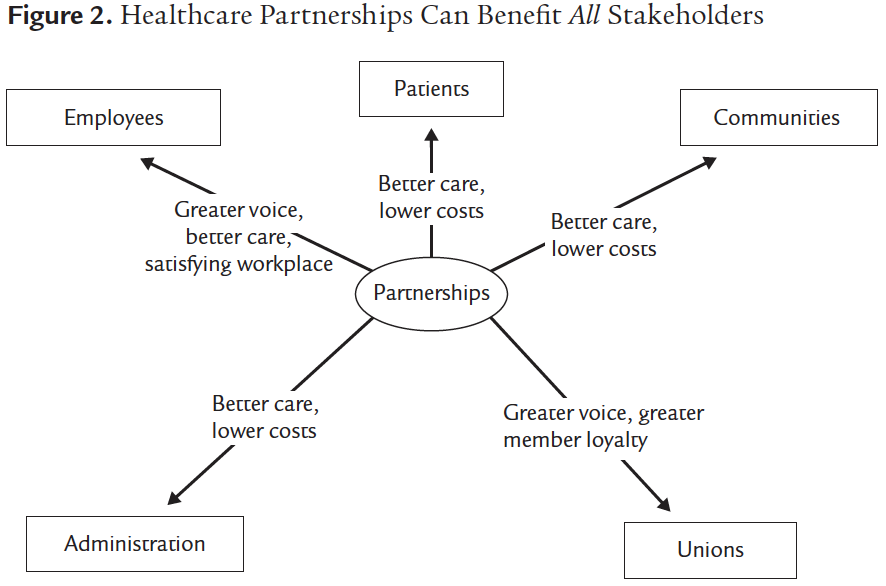
Examples of the use of Labor-Management Partnerships to structure a shared decisionmaking process among the organizational stakeholders are there when you look for them, and are provided throughout our new book, From the Ground Up. What we see, time after time, is that within such partnerships all stakeholders, including patients, contribute to and benefit from the process (see figure 2).
One example of a Labor-Management Partnership concerns the joint effort of administrators, nurses, physicians, and other staff in one hospital to respond to a series of sudden deaths that occurred within their cardiology unit over a short time period. The hospital administration’s initial response to this crisis was to penalize nurses who had not responded quickly enough to the patients’ cardiac monitors. A more forwardthinking response occurred when the hospital’s Labor-Management Partnership created a joint task force composed of clinical personnel on the unit and their departmental administrator to study what had actually led to these errors. As a result of their joint analysis of the crisis, the hospital eventually purchased a more effective cardiac monitoring system, and various practices surrounding the transport of monitored patients and the assignment of nurses to high-risk patients were instituted. As a result, no more such deaths occurred in subsequent years. The administration alone had not been aware enough of the practical difficulties in caring for and monitoring such patients to be able to arrive at such a solution by themselves.
Working together, administrators and frontline staff can claim responsibility for envisioning, researching, and implementing the changes necessary …
A CALL FOR COLLECTIVE ACTION
You never change things by fighting the existing reality. To change something, build a new model that makes the existing model obsolete. —Buckminster Fuller
As we were researching and writing our new book, many doctors and nurses confided in us their absolute distress over the way our healthcare system has shifted in the past 30 years, which they see as depriving them of the opportunity to practice clinical care in a meaningful, professional, and ethical manner. We view them as suffering from a sense of “moral injury.” Moral injury constitutes “the damage done to one’s conscience or moral compass when [a] person perpetrates, witnesses, or fails to prevent acts that transgress one’s own moral beliefs, values, or ethical codes of conduct.”[13] Originally observed by Jonathan Shay[14] in returning Vietnam War veterans, this phenomenon has been observed by some nurses and doctors within themselves: “The system had bound the physicians so tightly with scheduling control, data and metrics, policies and punishment that they … could barely breathe. They had almost no control over their patient interactions or their referral options … they knew what patients needed but did not have the latitude or the autonomy to get it.”[15] We need a call for collective action in the face of such forces, which have created powerful and disruptive incursions into the ability of professional staff to provide patients with the care they need. Patients are forced into the untenable situation of being treated by clinicians who are increasingly hamstrung in their capacities to provide them with personal, professional, and empathic care.
A severe but silent sense of injury dominates our healthcare system as currently constructed. Many administrators fail to recognize this, or when they do, they do not know how to enact meaningful change. Even when observed from a strictly corporate point of view, however, the top-down, siloed methods they use increase costs as well as offering inferior clinical outcomes. “Administrative creep”[16] has overwhelmed most systems, with 10 administrators hired for every physician and an increase in administrative hiring of 3200 percent from 1975 to 2010.[17] Significant costs have accrued from these skyrocketing administrative salaries, as well as from inefficient care processes.[18]
In order to create systems that provide cost-effective, timely, professional, and bettercoordinated care, it is essential that healthcare organizations make use of the input of staff at every level. This approach is endorsed by many who study complex organizational structures. It holds no matter what form of payment is used,whether a patient has insurance through his or her employer, exercises a public option, or is enrolled in Medicare for All. What is important is to find a payment process in which all Americans have access to healthcare services, healthcare systems are reimbursed for care coordination, and clinicians are not penalized for ethical practices.
Without hearing the voices of their staff, healthcare organizations lack clear-cut methods to fully identify systemic problems in clinical care. In fact, within many hospitals, clinician-employees feel hampered in voicing their concerns from fear of being reprimanded.[19] Fearing censure or dismissals, most practitioners don’t speak up.
Many use shortcuts such as workarounds, which may be effective in the short run but do nothing to resolve issues in work or care design. (A common example of a workaround is the borrowing of supplies and equipment from other units when they are missing in one’s own, or changing procedure coding to obtain payment for extra time spent with a patient.)
When staff, patients, and regulatory organizations are excluded from hospital initiatives for improving access and quality of care, the institution automatically loses essential input. When administrators purchase equipment or software such as electronic medical records systems without consulting with the clinicians who will use them, those clinicians flounder under the weight of the added workload. Electronic medical records, “intended as work-saving tools, have gone in the opposite direction, taking time away from patient care in the name of electronic box-checking.”[20] This results in frustration for all.
There are positive examples to follow. Maimonides Medical Center and the Los Angeles County Department of Health Services were extremely fortunate to have been graced with visionary leaders who deeply understood the value of collaboration with all of their staff. Senior administrators and union leaders such as Pam Brier and Bruce Richard at Maimonides, and Dr. Mitchell Katz and Patricia Castillo in Los Angeles, were aware of the importance of staff buy-in for the changes they anticipated to be essential for their centers, and they became convinced of the importance of working with their employees to fully identify and correct shortcomings in care.
When healthcare leaders, on the other hand, are cautious, unfamiliar with such methods, biased against labor-management collaboration, hostile toward labor unions, or simply unwilling to share their power, frontline staff and their local unions, such as the AFT’s Vermont Federation of Nurses and Health Professionals at the University of Vermont Medical Center, can exert pressure on them to change. While it is extremely difficult to challenge the power of the massive organizations that own chains of hospitals and of large private insurance companies, nonetheless the systems that have succeeded in these endeavors offer proof that collaborative organizational structures benefit hospitals, staff, patients, and the bottom line. These examples need to be trumpeted to all concerned: our political leaders, regulators, and everyone with a stake in the healthcare system. Healthcare partnerships benefit patients, staff, and administrators.
(We go into great detail on all of this in From the Ground Up.)
A highly structured form of collaboration, LMPs have been shown to successfully tackle systemic problems in healthcare organizations. Several essential practices contribute to their success. These practices include the following:
- Establishing a social contract between labor and management from the outset that outlines their goals and mutual responsibilities
- Developing extensive educational activities for frontline staff and senior leaders to familiarize them with the methods and importance of collaborative work
- Developing internal consultants to oversee and assist the teams charged with identifying and solving problems within the organization
- Attending to the overall tone and practice of labor relationships within the organization
- Stressing the importance of documentation and com-munication of the results of partnership activities
Labor-Management Partnerships have multiple options for approaching organizational change. These include developing teams of frontline staff who identify, analyze, and solve problems with clinical care in their individual units, department-based teams that address issues within an entire department, and Study Action Teams that focus on systemic issues within an entire medical center.
Once teams have been established, it is important for team leaders and internal consultants to be prepared to address the irrational forces that at times can overtake group functioning. Arming teams with knowledge about problem-solving techniques, conflict-resolution strategies, and the basics of workflow analysis will go far to prevent the kinds of irrational forces that can overtake groups when they are unstructured and unprepared for their task.
Nonetheless, it is useful for team leaders to be prepared to work through the impasses that sometimes arise within groups. At times, teams may engage in infighting or in blaming outside forces for their difficulties, may become passive and leave their leader to do all of their work, or may retreat into distracting, gossipy exchanges—all to the detriment of their functioning.
We also stress the importance of understanding and addressing the sensitive issues that arise within groups composed of members from different strata of the power hierarchy and of different ethnicities. In these instances, it is helpful to compose group membership in a way that guarantees that staff at the bottom of the hierarchy are well represented and heard. Group leaders should be coached to make sure that such members feel able to safely contribute their thoughts. Many times, meeting separately with these employees can be helpful in getting them comfortable to share ideas and to speak up in groups with other stakeholders, regardless of who they are.
Once systems have been persuaded to engage in Labor-Management Partnerships and their teams are effectively functioning, other strategies might be enlisted that further enhance workers’ autonomy and allow them to contribute to their organizations’ bottom lines. We have seen strategies employed in Europe and in the United States to encourage staff to develop innovative services, work processes, and technologies that may produce additional income for their hospital system, as well as expand their own job possibilities. Some universities have partnered with these efforts, sharing their own areas of expertise, such as in technology, product development, and marketing. In Europe, unions have actively financed such activities and championed them.
In many hospital settings in the United States, healthcare unions have unfortunately been excluded from exercising such opportunities or have resisted organizing their members to insist on meaningful and clinically ethical work practices. The unions who actively participated—in the Allegheny General Hospital, Kaiser Permanente, Los Angeles County Department of Health Services, Maimonides Medical Center, and University of Vermont Medical Center Partnerships, for example—created a voice for workers and improved the quality of their work lives. They also increased contact with their members and demonstrated their active value beyond contract negotiations and the handling of grievances. This resulted in increased union membership and increased power for the unions in these healthcare organizations. Many healthcare unions have now developed their own structures to assist in partnership efforts, and it is hoped that these will continue to be used.
ENLISTING HEALTHCARE MANAGERS AND ADMINISTRATORS INTO COLLABORATIVE WORK
We have already mentioned reasons for managers’ and administrators’ resistance toward partnerships and have discussed the need to exert pressure on them to consider this option. One of the dilemmas with which we have struggled has been to identify alternate approaches to senior managers that might help overcome their resistance to structured collaboration.
Most hospital and healthcare administrators, as well as managers of manufacturing and high-tech companies, lack knowledge about the benefits of structured collaboration as an effective management tool. Clayton Christensen, in his seminal book on what is needed to improve our healthcare systems, The Innovator’s Prescription, emphasizes that unfortunately “most of the current actors in the healthcare industry lack the scale and scope to create a new system architecture.”[21]
Healthcare managers have operated, to a large extent, by “keeping the trains running on time,” rather than by creating a vision about what troubles their organizations’ effective operation and researching methods to redress these. Many managers are low-risk-takers with handsome rewards that they are reluctant to sacrifice. The mean annual compensation for major nonprofit medical center CEOs is now over $3.1 million, 12 times more than pediatricians receive.[22] They tend to justify such salaries by surrounding themselves with the trappings of a power that they are reluctant to share.
It takes vision and courage for them to disrupt the current fee-for-service processes in order to demand that insurers reimburse activities that coordinate care or to insist that insurers alter their electronic medical records requirements to be more clinicianappropriate. As Steve Shortell at the University of California, Berkeley, School of Public Health states, “We are not yet at the tipping point of what is needed to improve healthcare quality or contain costs.”[23] Why risk rocking the boat with a new approach when healthcare administrators do not yet face the pressure that will force them to make systemic changes?
It is therefore imperative for organizations such as America’s Essential Hospitals, the Association of American Medical Colleges, the American Public Health Association, the American Management Association, and the Labor and Employment Relations Association to educate their constituents about the urgent need for systemic change.
These organizations have an obligation to educate themselves and their constituents about the data on successful organizational change methods.
Over the long term, nursing, medical, public health, and business schools should fulfill this obligation by including courses in organizational change, in methods to create new work systems, and in approaches to collaboration with frontline staff. This will help the next generation of healthcare leaders to become more open to and knowledgeable about such approaches to systemic change. Some healthcare unions, such as the Committee of Interns and Residents, the Doctors Council, and the American Federation of Teachers’ Nurses and Health Profes-sionals division, are already fulfilling this obligation by requiring their leaders to become educated about these methods.
In the near term, conferences and strategically placed articles and books, such as ours, can be used to encourage healthcare administrators to learn from their colleagues—Mitch Katz, Pam Brier, and others—about practical ways to restructure their operations. We have written about the reasons why groups tend to hold negative mindsets toward “the other,” “the outsider.” Such prejudices can powerfully influence leaders against collaboration. These stances might be affected, however, by their hearing firsthand from peers about actual, positive experiences and their beneficial results.
Apart from emphasizing the intrinsic benefits to healthcare organizations of working collaboratively with their frontline staff, we hope that public health educators will also stress the benefit of such work to their communities. Several studies document that after participating in frontline staff decision-making activities, employees were much more likely to become actively engaged in civic projects outside of work. This is a highly desirable benefit, as it can strengthen our democratic institutions, which are currently in peril.
In the end, however, the American healthcare “system” is entangled by corporate greed. Pharmaceutical companies feel entitled to jack up prices for medications that are essential to patient care, even when they have been previously available at low cost. Private insurers regard their primary responsibility as meeting their shareholders’ needs and as accruing their own profits, rather than as providing a service to their enrolled patients.
According to a review of Elizabeth Rosenthal’s book An American Sickness, “Even nonprofit Medic-are and Medicaid now contract out services to some [private insurers whose] many tangled plans and subplans have providers bouncing on and off their rosters at warp speed, destroying continuity of care. … Likewise, medications flit on and off approved drug lists, their presence or absence depending on continual negotiations between insurer and manufacturer.”[24] As for “nonprofit” hospitals, they often funnel their gains into large executive salaries and new wings or buildings instead of staff salaries and patient care.
It will require collective action on the part of healthcare practitioners and patients to insist on disentangling the tentacles of these highly intertwined systems. Rather than giving in to misery or simply leaving the field, these groups must learn that it is up to them to demand change.
We offer in our book a blueprint for one way of reversing the trends of the last 30 years that have strangled our patient care systems. Hopefully, collective action by those with a stake in actually treating patients (rather than simply enriching themselves), in synchrony with political change, can help to resurrect a viable American healthcare system.
It is likely that a single-payer coverage system with secondary supplementation for copayments, added drug coverage, and comprehensive behavioral health benefits will create a situation in which everyone will be insured. In this way, coverage will no longer be subject to the Byzantine sign-up conditions and high deductibles of the Obamacare plan and will not be held hostage by for-profit companies. It should also be easier to negotiate costs and conditions, given enough pressure from all stakeholders, with a single entity, as opposed to with multiple players. We await the tipping point at which this will become possible. We hope, given the chaos surrounding patients’ coverage throughout the COVID-19 epidemic, that the tipping point may have arrived.
Adapted from From the Ground Up by Peter Lazes & Marie Rudden. Copyright © 2020 by Peter Lazes and Marie Rudden.
All rights reserved. No part of this excerpt may be reproduced or reprinted without permission in writing from the publisher.
ABOUT THE AUTHORS
Peter Lazes, PhD, is the founder and former director of Programs for Employment and Workplace Systems and of the Healthcare Transformation Project, both at Cornell University. For over forty years, he has been dedicated to designing systems in which the knowledge and experience of frontline staff are used to improve patient care and to save the jobs of American workers.
Marie Rudden, MD, is a psychoanalyst and clinical assistant professor in psychiatry at Weill Cornell Medicine and an associate editor for the International Journal of Applied Psychoanalytic Studies. Rudden is also on the North American Editorial Board of the International Journal of Psychoanalysis and is a training and supervising analyst at the Berkshire Psychoanalytic Institute.